The clinical identification of keratoconus has traditionally relied on mapping the physical shape of the eye. Over several decades, technology has moved from basic measurements to high-resolution imaging that allows clinicians to see minute changes in corneal curvature and thickness. However, a central question persists: does the cornea’s structural integrity fail before its shape begins to change? If the weakening of the corneal tissue is the first step in the disease process, relying solely on shape-based imaging might mean we are missing the earliest window for intervention.
The Limitations of Current Imaging
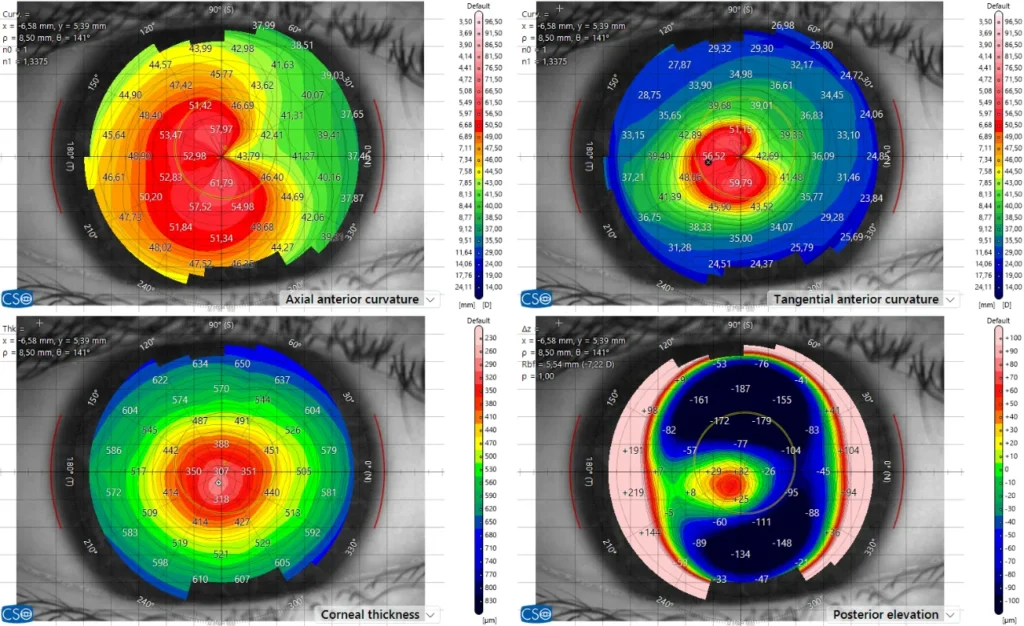
In most clinics, we look for specific physical signs of keratoconus: a thinning of the cornea or an abnormal bulge on its surface. While these tools are highly accurate at identifying established disease, they are less definitive in “borderline” cases. In these instances, the images show the current state of the eye but cannot easily predict whether the tissue will remain stable or deteriorate over time.
Integrating biomechanical assessment into clinical practice is an attempt to fill this gap. By using a controlled pulse of air and high-speed imaging, researchers can measure how the cornea deforms and recovers. This provides data on the stiffness of the tissue. The scientific challenge is to determine if these measurements provide new, independent information, or if they simply reflect the thinning that we can already see on standard scans.
The Uzbekistan Clinical Study
To investigate this, under the auspices of the Light for Sight Foundation, researchers from the ELZA Institute and Andijan State Medical University in Uzbekistan have begun a study involving both adults and children. By using both tomography (to measure shape) and biomechanical analysis (to measure strength), the research group is looking for a quantifiable link between tissue weakness and irregular corneal shapes.
The inclusion of children is a critical part of this research. Because keratoconus often progresses more rapidly in younger patients, finding a way to detect instability before the cornea actually deforms is a high priority. If the study shows that biomechanical weakness can be caught before the shape changes, it could change how we screen for the disease in high-risk populations.
Considering the Evidence
There is a clear biological reason to look at tissue strength. We know that keratoconus involves a breakdown of the corneal matrix. However, turning this biological fact into a reliable clinical test is difficult. Factors like the internal pressure of the eye can interfere with measurements of tissue stiffness, making it hard to get a “pure” reading of the cornea’s strength.
Additionally, we have to consider the practical impact of new screening methods. While earlier detection is the goal, any new test must be accurate enough to avoid high rates of false positives, which can cause unnecessary worry for patients. The data from the Tashkent and Andijan study will help clarify where the threshold for “at risk” should actually be set.
Next Steps in Screening
The work being done in Uzbekistan is an effort to move diagnostic standards away from late-stage indicators, like loss of vision, toward an earlier understanding of tissue health.
It is not yet certain if biomechanical testing will become the primary tool for detecting keratoconus. Current evidence suggests it is a useful addition to our existing tools, but more long-term data is needed to prove it can stand alone as a predictive test. As the ELZA Institute continues this research, the focus remains on whether we can move from simply observing the shape of the eye to accurately measuring its underlying stability.