The word “cataract” comes from the Greek for “waterfall”, καταρράκτης, as rapidly flowing water in waterfalls appears to be white, just like advanced cataracts appear in the eye.
The most common cause of cataract is that as you get older, the lenses of your eyes gradually become less transparent, which is a natural consequence of ageing. The first symptoms of cataracts are vision problems at dusk, such as blur, haze and glare, and the need for more light to read. If left untreated, cataracts become increasingly cloudy and dense, which can ultimately reduce vision to a point where a person becomes blind. Fortunately, cataract surgery enables people to regain their vision. Thereby, the cloudy lens is replaced with a new artificial intraocular lens (IOL). Modern cataract surgery and advanced, premium IOLs can correct for many other vision disorders like long or short-sightedness and astigmatism, so in many cases patients have the option to become far less reliant on wearing spectacles after the surgery.
As cataracts are not exactly a disease, but rather part of the normal ageing of the body, it is very common amongst the population above the age of 50. 1 in 5 people aged between 65 and 74 have cataracts, and above this age, the proportion rises to 1 in 2.
Cataract is a progressive clouding of the eye lens. Every person will one day go on to develop a cataract if he or she gets old enough. Some people develop a cataract at the age of 45, others at 85. This depends primarily on how much ultraviolet light the eye has been exposed to in the course of life, and especially in youth. People from sun-rich countries, such as those around the Mediterranean sea, often develop a cataract in their mid-fifties. Cataract is therefore not a disease, but a natural symptom of aging.
A healthy lens is clear, but in a cataract, the lens of the eye gradually becomes harder as well as cloudier, allowing less light to pass, making it harder to see. If we compare the natural lens with the lens of a camera, one can say that the lens is severely scratched and clouded. The result is a bad, blurry and cloudy image.
Although relatively easy to remedy by surgery, cataract is the most common cause of blindness in the world, as in poorer countries most people can not afford such an operation.



Ageing is responsible for around 90% of cases of cataract but there are several other risk factors that can cause cataract or contribute to its formation.
Very occasionally, children are born with cataracts, often to mothers who are infected with measles or rubella during pregnancy.
As the lens ages with the years, just like the rest of the body, almost every person will eventually get cataract. However, there are a number of steps you can take to slow the development of cataracts. These mainly include avoiding the risk factors:
Avoid exposure of the eyes to UV-light, e.g. by wearing sunglasses on sunny days. Good sunglasses block UV light from reaching your eyes, which is especially important at a young age.
Smoking accelerates the ageing process – and this includes cataract development.
If you have to take corticosteroid drugs for a long time, consider asking your doctor if there are non-steroid alternatives that you can take instead.
If you are not already vaccinated against measles and rubella, consider doing so before becoming pregnant, as these diseases can cause cataract in the unborn child.
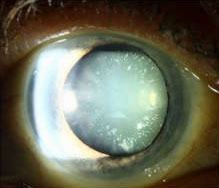
The first stages of cataract formation are often not noticeable. However, vision slowly gets worse, and images start to become blurry. People usually first notice this at dusk, as glare, halos and blurring are most noticeable. People often describe their vision as looking through fog, and people tend to report needing more light in order to read.
As your cataract continues to develop, your contrast sensitivity starts to get worse, making it harder to read texts, that are not pitch black on white. If the cataract is advanced enough, it can eventually be seen through the pupil of the eye, as a grey, cloudy substance. At this point, a person is close to blindness.
Read more…




The clouding of the lens itself cannot be reversed. However, it is very well possible to remove the cloudy lens and replace it with an artificial intraocular lens (IOL). This is a very quick surgery, which immediately eliminates the symptoms you have due to the cataract. Nowadays, there are many different types of intraocular lenses, and choosing the right one for you is crucial. If a cataract has been diagnosed we carefully evaluate the right time for the procedure, as well as the right IOL and type of surgery. Many measurements of your eye are made in order to calculate the “refractive power” that your eye needs.
Please remember, that the cataract might not be the only factor in the eye that reduces the visual acuity. The surgery might therefore provide a person with a better vision, but still not with 100% visual acuity.
Cataract is diagnosed and graded by an eyecare professional. If it is medically necessary to do the surgery (e.g. in very advanced cases, if the cataract poses a risk to the eye), the doctor will recommend it. If it is medically not necessary yet, the choice on when to do the surgery is mainly based on how much a patient is restricted and disturbed by the decreased vision.
Cataract surgery is a day surgery and usually takes about 20 minutes per eye. The operation is performed under local anesthesia with light sedation and assisted ventilation under the supervision of an anesthesiologist. General anesthesia is necessary only in exceptional cases.
The natural, cloudy lens of the eye sits in a capsular bag. Under the microscope, this capsule must be opened so that the lens can be broken into smaller pieces and removed. In order to reach the lens with the instruments, three small incisions are made at the edge of the cornea. The artificial clear lens (intraocular lens, IOL), which will take over the function of the normal human lens, is then also inserted through these.
There are two main ways of performing cataract surgery: manually, and with a femtosecond laser.
In manual surgery, the incisions in the cornea to introduce surgical instruments and the new lens, are performed manually by the surgeon. Then the surgeon uses an instrument to tear a hole in the capsular bag that contains the lens; this process is called capsulorhexis. The surgeon then liquifies and breaks down the lens with ultrasound energy in a process called phacoemulsification, and removes the lens fragments through suction. The new lens is placed into the bag through the circular hole, and the optical part of the lens is positioned so it fits in the middle of the hole.
Femtosecond laser surgery involves the use of a laser to make all of the incisions with micrometer precision, as well as making a perfectly circular opening in the capsular bag to place the lens inside. Furthermore, the laser pre-cuts the cloudy lens, so that less ultrasound-energy is required to break down the lens. This is important because too much ultrasound energy can damage the cells at the base of the cornea.
The precision of the laser ensures that the lens fits as perfectly as possible in the hole, and some premium lenses require an extremely precise fit.
Read more…
Monofocal lenses are an excellent option and give you a good vision at one distance, if your eyes are otherwise healthy. The distance, where the clear image is, can be chosen and usually lies in the far distance. Spectacles / reading glasses will be necessary for you to see at other (closer) distances.
Multifocal lenses involve splitting the light that comes into the eye into two or more sharp images, e.g. near and far, or near, intermediate distance, and far. Your brain then chooses the image you want to see in focus. The trade-off is that incoming light is split between the images, and this reduces your contrast sensitivity (although it will be better than before surgery).
Extended depth-of-focus (EDOF) IOLs use specialized optics to spread the sharp image focus along a greater range of distances. Again, this can come with the drawback of reduced contrast sensitivity, and depending on the design of the lens, glares and halo.
Toric lenses are designed to also correct for any astigmatism in your eye. These exist in monofocal, multifocal and EDOF forms.
Read more…
 Aspheric
Aspheric
 EDOF
EDOF
In some circumstances, the implantation of special (multifocal) lenses that allow close and distant vision is also possible. To find out whether this is the case with you, the doctor will talk to you directly during the preliminary examination.
In principle, this is possible, but is done only in exceptional cases, as unnecessary operations should be avoided. However, if the lens exchange is indeed necessary, then this can be done in a short intervention.
Ophthalmology now has over 50 years of experience in the materials used to make the lenses. A modern intraocular lens lasts a lifetime.
No. Despite the high quality standards, the prices of the ELZA are the same as in a public hospital.
Yes. The services are uniformly regulated throughout Switzerland, whether you live in Geneva or Chur.
No. At most, something called “posterior capsule opacification” can develop, but this can be removed easily with a laser, on an outpatient basis, without having to reopen the eye.
Yes, today we can gently treat the cataract with a femtosecond laser. The removal of cataract by femtosecond laser is the most advanced method of cataract surgery and we use it regularly. However, it is not yet covered by Swiss health insurance companies.
Patients often assume that a cataract must be well advanced before surgery is necessary. This is not correct. If your ophthalmologist sees signs of cataract and you start to notice visual disturbances, you should ask your ophthalmologist about the options available to you before it starts to affect your quality of life.
Left untreated, the cataract progresses. Your lens becomes increasingly opaque. The rate at which cataracts develop varies from person to person, but the end result is always the same: once the lens is completely clouded, the result is blindness. Furthermore, more advanced cataracts are more difficult to remove: the surgery takes longer and the risk of complications rise, so it’s important not to wait too long for surgery.
In most cases, the operation is performed by means of a local anesthesia with eyedrops. General anasethesia is very, very rare in cataract surgery, and is used only in very special cases.
Yes. If necessary, your surgeon will also provide you with painkillers and medicines to help you relax during the procedure.
The surgery itself typically lasts between 15 and 30 minutes. However, if you add up the total time you spend with us (preparation, surgery, rest afterwards), the entire process takes between 2–3 hours.
No. Make-up near the eye (especially eyeliner and mascara) may contain pigment particles as well as bacteria. We ask that you do not use make-up three days before surgery and two weeks after surgery
No. Continue with all medications until the day before surgery as normal. Do not use eye drops in the eye that will be operated on the day of surgery. Eye drops for the other eye can be used as normal.
Please do not eat any food for at least 4 hours before the operation, however, a cup of tea on the morning of the operation is allowed.
The choice of artificial, or intraocular lens (IOL), that patients receive during cataract surgery depends on their lifestyle and their visual needs. Your surgeon will make a clear recommendation based on your stated needs. However, it is recommended that patients understand what monofocal, multifocal lenses, and toric lenses are and how they work before this meeting.
This would be easier. The painkiller we give you may make you feel dazed, which can make using public transport problematic.
You’re usually ready to return to work within one week, and in rare cases, two weeks.
In the first week, you can run the shower, ensuring that no water gets in your eyes. You can apply make-up after 2 weeks – but you must take care not to rub when removing make-up, only dab. Sporting activity is possible again after two weeks, but please avoid exerting yourself for the first six weeks (i.e. no red cheeks from effort). The same applies to the lifting of heavy objects.
Pain after surgery is rare. We give you painkillers. If pain persists you should contact the surgeon.
The answer will vary from case to case and will be discussed with you by the surgeon. Often we leave 2 weeks between the eyes.
The follow-up appointments are usually one and two days after the operation, followed by one week, one month and three months.
Due to the healing of the eye, it can take 12 weeks before vision has finished stabilising, at which point we can make a definitive spectacle prescription, but in many cases, it is possible to fit a provisional lens after about 1 week. In Switzerland, the post-surgery spectacle lenses are covered by the so-called “MIGEL list”.
All necessary eye drops are given to you after the operation. As a rule, eyedrop therapy lasts four weeks.
Low pain and mild nausea may occur after surgery. In case of severe pain, please contact the surgeon immediately. The emergency number will be communicated to you on the day of the operation.
Vision in the first few days after the operation may be impaired. This is usually not permanent. If any further action is required, the surgeon will discuss this with you directly.
Get in touch
During office hours.
Email us.
Make an appointment, and come to see us.
Thank you for writing a review on google.
Contact us here, we will get in touch with you.
Zoom online consultation for our international patients.
Contact us here, we will get in touch with you.
Contact us here, we will get in touch with you.
Stay informed & get the newsletter
You have successfully joined our subscriber list.
Newsletter abonnieren & informiert bleiben
Sie haben sich erfolgreich in unsere Abonnentenliste eingetragen.
Bitte bestätigen Sie Ihr Abonnement, indem Sie auf den Link in der E-Mail klicken, die wir Ihnen gerade geschickt haben.