
Cataract surgery in patients with keratoconus presents challenges that extend well beyond routine cases. A recent clinical review in ophta by Dr. Emilio Torres-Netto MD, PhD, FEBO, FWCRS, examines how corneal irregularity, altered ocular biometry, and disease stage affect intraocular lens (IOL) calculation, surgical planning, and postoperative outcomes. The article emphasizes that successful cataract surgery in keratoconic eyes requires an individualized, expectation-managed approach rather than reliance on standard workflows.
Accurate IOL power calculation is a central difficulty. In keratoconus, corneal refractive power is highly variable and often decentered, while axial length tends to be longer than in normal eyes. Irregular astigmatism, higher-order aberrations, tear film instability, and poor fixation can further compromise biometry reliability. Additionally, posterior corneal steepening alters the anterior–posterior curvature ratio, leading to overestimation of corneal power and a tendency toward postoperative hyperopic error.
No single IOL calculation formula performs reliably across all stages of keratoconus. While early disease may allow acceptable accuracy with modern fourth-generation formulas, predictability declines markedly in moderate and advanced cases. The review recommends comparing multiple formulas, using different keratometric inputs, and acknowledging the inherent imprecision of all current methods. Keratoconus-specific formulas may assist in selected cases but remain limited at higher keratometric values.
Lens selection should remain conservative. Monofocal IOLs are generally preferred, with monofocal toric lenses considered only in carefully selected eyes with relatively regular central astigmatism and no intention to resume rigid contact lens wear. Multifocal, EDOF, or other complex IOL designs are discouraged due to the optical instability of keratoconic corneas. Target refraction is typically mild myopia to offset the frequent hyperopic shift observed postoperatively, particularly in more advanced disease.
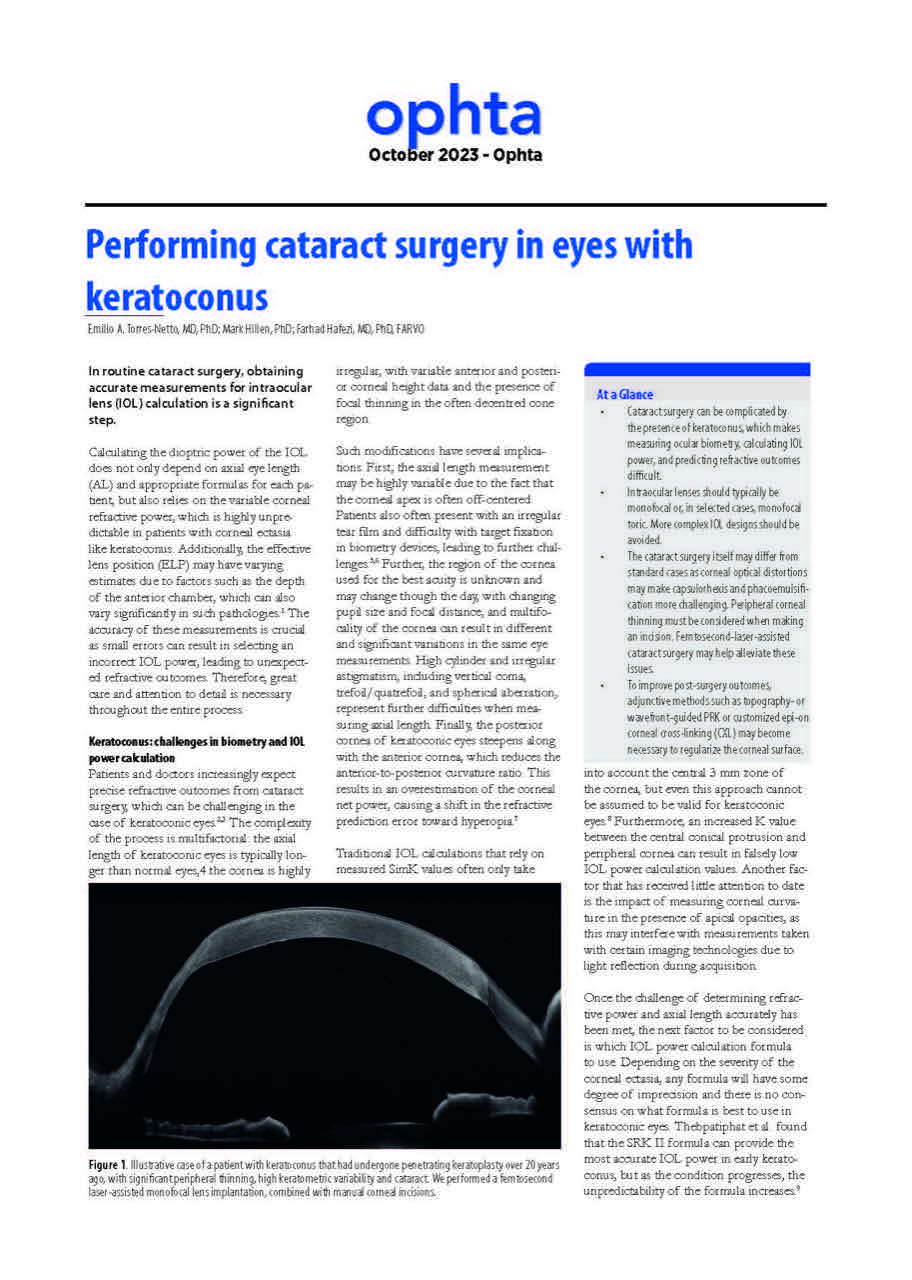
From a surgical perspective, cataract extraction in keratoconus often resembles standard phacoemulsification but requires attention to peripheral corneal thinning, incision placement, and intraoperative pressure control. Femtosecond laser–assisted cataract surgery may facilitate capsulorhexis and lens fragmentation in eyes with corneal distortion or opacity.
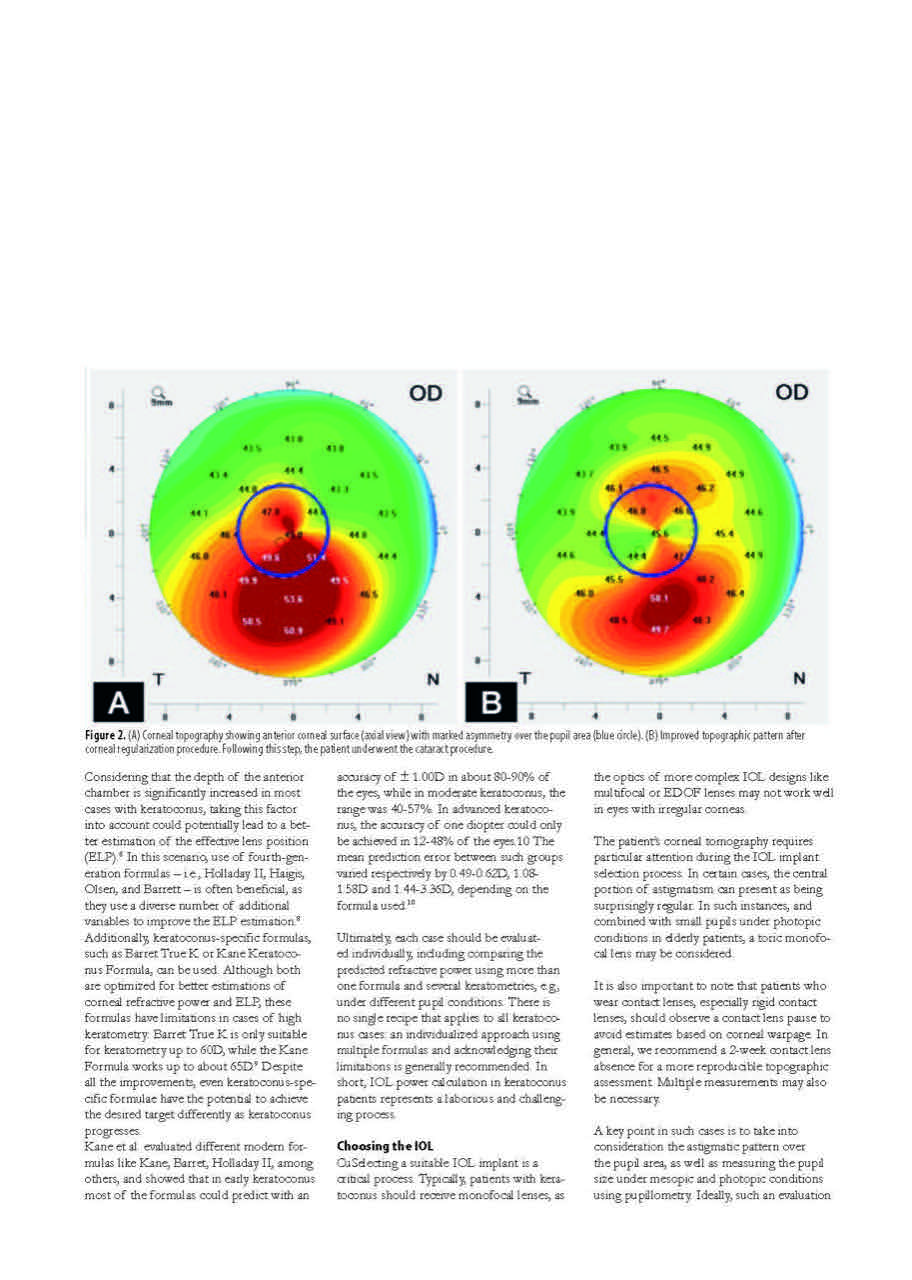
The article highlights the importance of corneal optimization strategies. In selected patients, corneal regularization—using procedures such as wavefront-guided surface ablation, intrastromal allogenic ring segments, or customized corneal cross-linking—may be performed before cataract surgery to improve biometry accuracy and visual outcomes. Timing depends on corneal stability, disease severity, and patient-specific visual goals.
At the ELZA Institute, cataract surgery in keratoconus is approached as part of a staged, cornea-first strategy when indicated. The reviewed evidence underscores that careful planning, realistic counseling, and individualized sequencing of corneal and lenticular procedures are essential to achieving clinically meaningful outcomes in this complex patient group.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
