The first distinction to be made is the difference between an inflammatory swelling in the eyelid area and “more tissue”. Eyelid tissue is delicate and a slight inflammation can lead to a massive swelling, and there can be many causes of this inflammation, including an inflamed lacrimal gland or an infection caused by a small injury.
If there is a real “extra tissue” (such as from a tumor), then it is often benign changes such as an encapsulated barley grain, a wart, or a so-called “molluscum contagiosum”, caused by a harmless, but contagious virus.
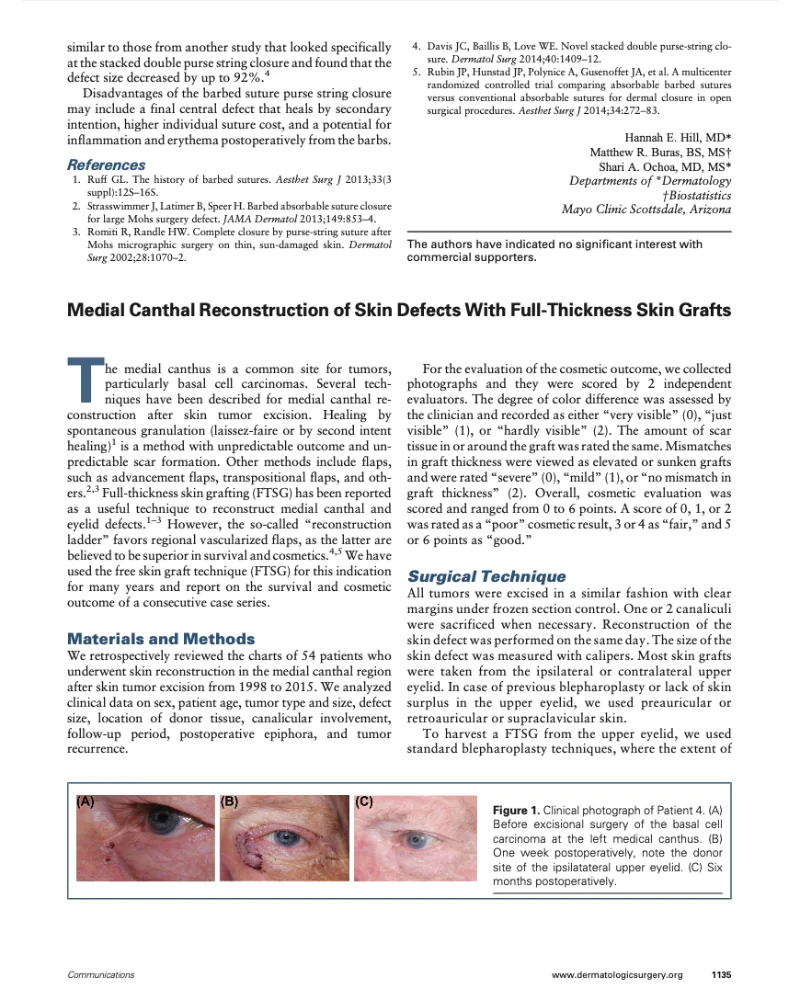
However, various malignant tumors (carcinomas) do occur on the eyelids. The most common malignant eyelid tumor is basal cell carcinoma (90%), followed by squamous cell carcinoma (~5%) and sebaceous carcinomas (~5%). In all cases, suspected malignant tumors should be treated quickly. If necessary, we will consult specialists of other disciplines such as internists, dermatologists or oncologists (cancer specialists).

 After
After
 Before
Before
 After
After
 Before
Before
 After
After
 Before
Before