Corneal cross-linking (CXL) is widely established as a biomechanical treatment for keratoconus and other corneal ectasias. Its role in infectious keratitis, however, remains an area of active investigation and debate. A recent expert roundtable published in EyeNet Magazine brings together clinical and research perspectives on when, how, and whether photoactivated chromophore–based cross-linking should be used in infectious corneal disease.
The rationale for CXL in infectious keratitis extends beyond corneal stiffening. In addition to increasing biomechanical resistance, CXL enhances stromal resistance to enzymatic digestion, generates reactive oxygen species, and induces photochemical damage to microbial DNA and RNA. These effects are particularly relevant in severe infections associated with corneal melting, where structural degradation rather than microbial load alone threatens globe integrity.
Clinical outcomes reported in the literature have been inconsistent, largely due to heterogeneity in study design, causative organisms, and—critically—treatment protocols. Much of the early clinical work relied on the standard Dresden fluence of 5.4 J/cm². Experimental data discussed in the roundtable indicate that higher fluence levels (10–15 J/cm²) produce substantially greater antimicrobial effects, with exponential increases in microbial kill rates observed in laboratory models.
Efficacy also appears to depend strongly on the causative organism and the chromophore used. Riboflavin-mediated CXL shows greater activity against bacterial pathogens, whereas rose bengal–based photodynamic approaches demonstrate superior effects against fungi and possibly Acanthamoeba, albeit with more superficial penetration. Differences in absorption spectra and stromal penetration depth complicate direct comparisons and underscore the importance of protocol selection.
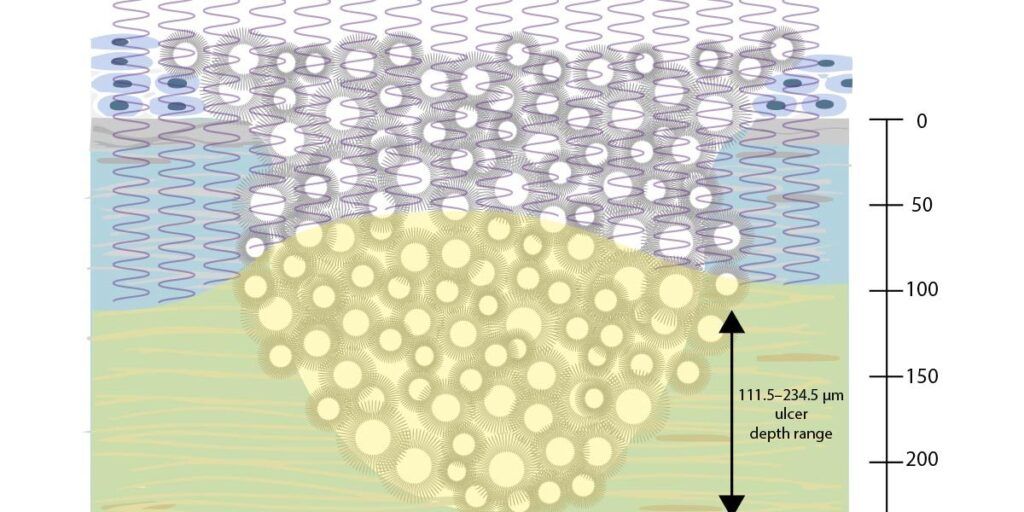
A key concept emphasized in the discussion is PACK-CXL (photoactivated chromophore for keratitis–corneal cross-linking), a term deliberately chosen to reflect flexibility in chromophore choice rather than reliance on riboflavin alone. Emerging experimental and early clinical work suggests that combining chromophores, such as riboflavin and rose bengal, at higher fluences may enhance resistance to enzymatic digestion and improve infection control in selected refractory cases. However, these approaches remain investigational and require careful consideration of endothelial safety and ulcer depth.
Importantly, all panelists agreed that, at present, CXL should be regarded as an adjunct to antimicrobial treatment in infectious keratitis rather than a replacement for it. Timing appears critical: earlier intervention in superficial, non-viral ulcers may improve outcomes, whereas advanced, deep, or viral infections carry higher risks and less predictable benefit.
At ELZA, CXL-based approaches for infectious keratitis are considered within a structured, evidence-informed framework that prioritizes organism type, ulcer depth, and safety margins. The roundtable reflects the current state of the field: promising mechanistic rationale, evolving protocols, and the need for rigorously designed, fluence-appropriate clinical trials before broader adoption.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
