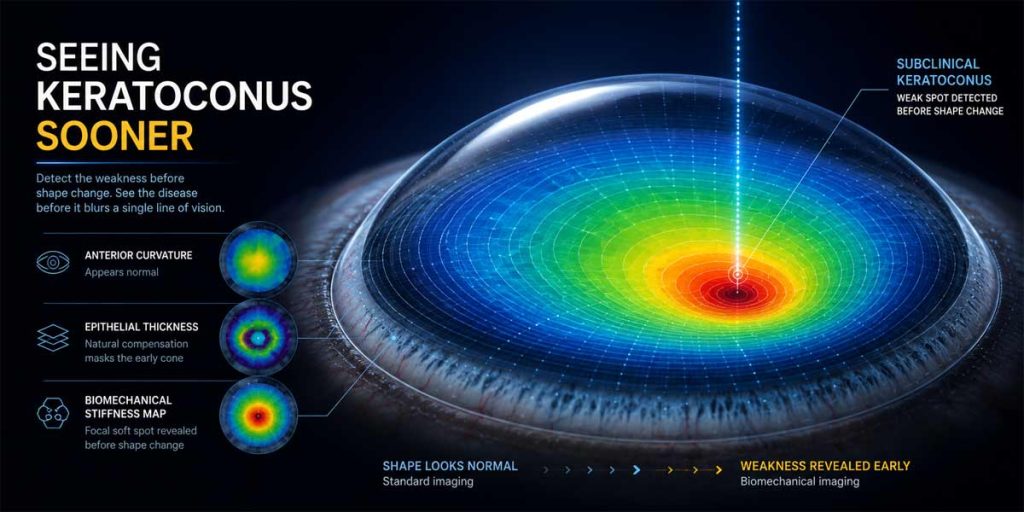
Seeing Keratoconus Sooner
The earliest sign of keratoconus may not be a change in shape at all — but a change in stiffness. Here is how corneal imaging is learning to catch the disease before it blurs a single line of vision.
Keratoconus is far easier to control when it is caught early — before the cornea has thinned and bulged enough to blur vision. Catch it late, and you are managing distortion, scarring and, in the worst cases, a corneal transplant. Catch it early, and a single, minimally invasive treatment can often stop the disease in its tracks. The difference between those two futures comes down almost entirely to imaging.
The hardest cornea to read is the one that looks normal. A cone in its earliest phase — so-called subclinical or forme fruste keratoconus — can pass a standard eye test, sail through a routine topography scan, and still be quietly on the move. Nowhere does that matter more than in screening candidates for laser vision correction, where treating an eye with a hidden weakness can tip it into ectasia. For decades the challenge has been the same: how do you see a problem that has not yet changed the shape of the eye?
Measuring stiffness, not just shape
The most intriguing answer on the horizon does not measure shape at all. It measures stiffness.
Keratoconus is, at its core, a biomechanical disease: the cornea weakens before it deforms. Standard topography and tomography capture the deformation — the steepening and the thinning — which means they are, by definition, reading the consequence rather than the cause. Brillouin microscopy goes after the cause directly. Using a phenomenon called Brillouin light scattering, it gauges the elastic properties of tissue at focal points throughout the cornea, without ever touching the eye, and builds a three-dimensional map of how stiff, or how soft, each region is.
In early keratoconus that map lights up a focal soft spot: a weakened patch surrounded by tissue that still looks, and measures, entirely normal on conventional scans. In a widely discussed study led by J Bradley Randleman, motion-tracking Brillouin microscopy separated eyes with subclinical keratoconus from healthy controls with perfect accuracy — 100 per cent sensitivity and specificity — outperforming every Scheimpflug metric in the same cohort. On the two-dimensional maps, the difference was visible to the naked eye.
It is worth being clear-eyed about where this stands. The devices are still largely custom-built, scans take minutes rather than seconds, and the studies so far are small. Brillouin microscopy is not yet sitting in your local clinic. But the principle behind it is a genuine shift: imaging that reports the weakness itself, not the shape change that eventually follows. EuroTimes has covered the emerging clinical data in detecting subclinical keratoconus.
What today’s imaging already catches
You do not, however, have to wait for Brillouin to catch a cone early. The imaging already in clinics has quietly become very good indeed.
The first generation of devices measured only the front surface of the cornea — topography, essentially a contour map of curvature. Today’s Scheimpflug tomography, such as the Pentacam, and OCT-based systems build a full three-dimensional model that adds the back surface and maps thickness from centre to edge. That extra dimension matters, because keratoconus often shows on the posterior surface first. Getting these foundational measurements right is a discipline in itself, as we explain in getting the basics of topography right.
The early-warning layer
One of the most useful advances is quieter still: epithelial thickness mapping. The eye’s surface epithelium is a natural camouflage artist. Faced with an early cone, it thins over the apex and thickens around it, smoothing the surface and masking the bulge underneath — which is exactly why a front-surface scan can look reassuring when it should not. That remodelling leaves a tell-tale fingerprint, and combined OCT/Placido devices such as the MS-39 make the pattern visible. In effect, the epithelium becomes an early-warning system, if you know how to read it.
Turning scans into decisions
Raw scans only become decisions through analysis. Displays such as the Belin/Ambrósio enhanced ectasia index distil dozens of measurements into a single risk score, and machine-learning models are increasingly able to separate truly progressive disease from stable corneas. That is how a clinician decides who needs cross-linking now and who can safely be watched. EuroTimes has explored this shift in a new era for keratoconus diagnostics.
Why earlier changes everything
All of this points in one direction. The sooner a cone is seen, the smaller the intervention needed to stop it — and the more vision the patient keeps. That is the logic behind the screen-and-treat-early approach championed by the Second Global Consensus on Keratoconus: find the disease while it is still a soft spot on a map, not a scar on the visual axis.
Whether the future belongs to biomechanical maps, smarter algorithms, or — most likely — both working together, the goal is the same one that has always driven the field. See keratoconus sooner, and you change how the story ends.
