PACK-CXL

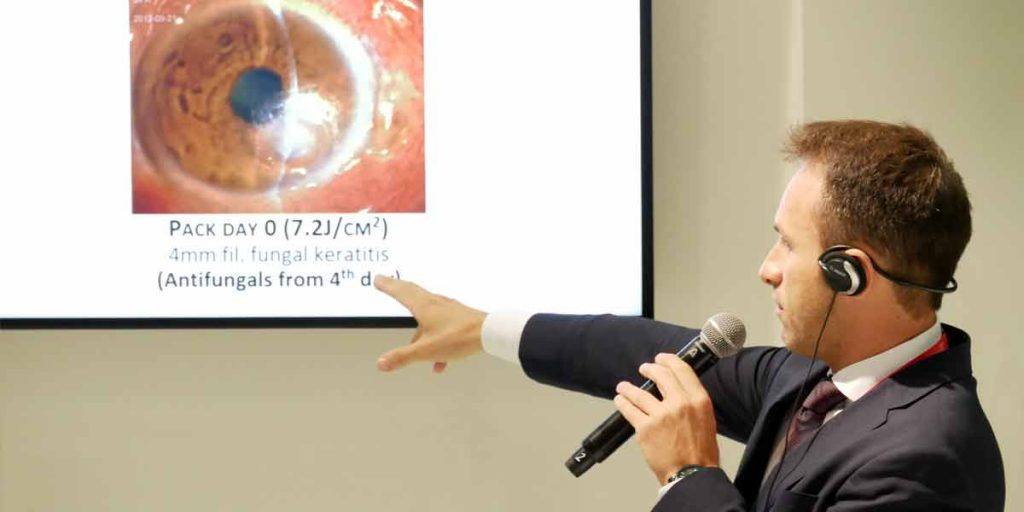
The process of cross-linking the cornea involves two important antimicrobial actions. The first is a direct, pathogen killing effect: UV illumination not only can kill pathogens, but the photoactivation of riboflavin into an excited state leads to it reacting with ambient oxygen, creating reactive oxygen species, which can also damage microbial DNA and cytoplasmic membranes. The second effect is a side-effect of the stiffening of the cornea: the additional cross-links between the (mostly collagen) molecules in the stroma makes the tissue more resistant to microbial enzymatic degradation – and therefore harder for the disease to spread. This use of cross-linking for the treatment of infectious keratitis has been termed “photoactivated chromophore for keratitis”, or PACK-CXL, and has shown great promise in treating corneal infections in clinical evaluations to date.
Customized cross-linking
As CXL can flatten the cornea, and the cornea is responsible for about 80% of the eye’s focusing power, as laser refractive surgery has shown with great success, changes in the shape of the cornea can correct refractive errors. In non-keratoconic eyes, customized cross-linking has been evaluated for the correction of small refractive errors, with a mean reduction of <1 D in hyperopia and myopia being observed after 1-year of follow-up.
Three-dimensional finite element analysis modelling of the keratoconic cornea has indicated that there is a differential biomechanical weakening of corneal tissue in the cone, suggesting that smaller-diameter, cone-centric treatments should result in a greater reduction of corneal curvature, and initial studies have suggested that this approach results in “somewhat greater reduction in maximum keratometry than with conventional cross-linking.”
Keratoprosthesis
The Boston Keratoprosthesis (Kpro) is a widely-used artificial cornea that’s used to treat corneal diseases that can’t be treated with penetrating keratoplasty or a corneal transplant. It consists of a corneal graft with a central hole in which an artificial optic part is placed through it and affixed to a base plate. However, the graft tissue is prone to corneal melts and tissue degradation, and cross-linking has been used to pre-treat the donor carrier tissue before it is used in Boston Kpro surgery in order to make the donor tissue more resistant to degradation.

The three key components of the Boston Keratoprosthesis (Kpro): optic, corneal graft and base plate. Cross-linking the corneal graft can help resist corneal melts and tissue degradation that sometimes occurs in Kpro implantations
Conclusion
Just like 20 years ago, the current gold standard for performing CXL to treat progressive keratoconus is the Dresden Protocol – both inside and outside the USA. However, this status quo might not remain in place for much longer; advances in our understanding of the photochemical reaction involved in cross-linking could mean that newer protocols and treatment regimens could supplant the Dresden protocol are on the horizon. Further, CXL has an expanding list of indications from treatment of corneal ectasia to infectious keratitis, and newer protocols, treatment regimens, and expanded indications look to be on the horizon. Watch this space.