The January 2026 issue of Cataract & Refractive Surgery Today presents a reflective case-based discussion examining how the management of early keratoconus has evolved over recent years. The article contrasts clinical decision-making in 2018 with contemporary practice, highlighting how advances in diagnostics and corneal cross-linking (CXL) strategies have reshaped treatment thresholds—particularly in pediatric and adolescent patients.
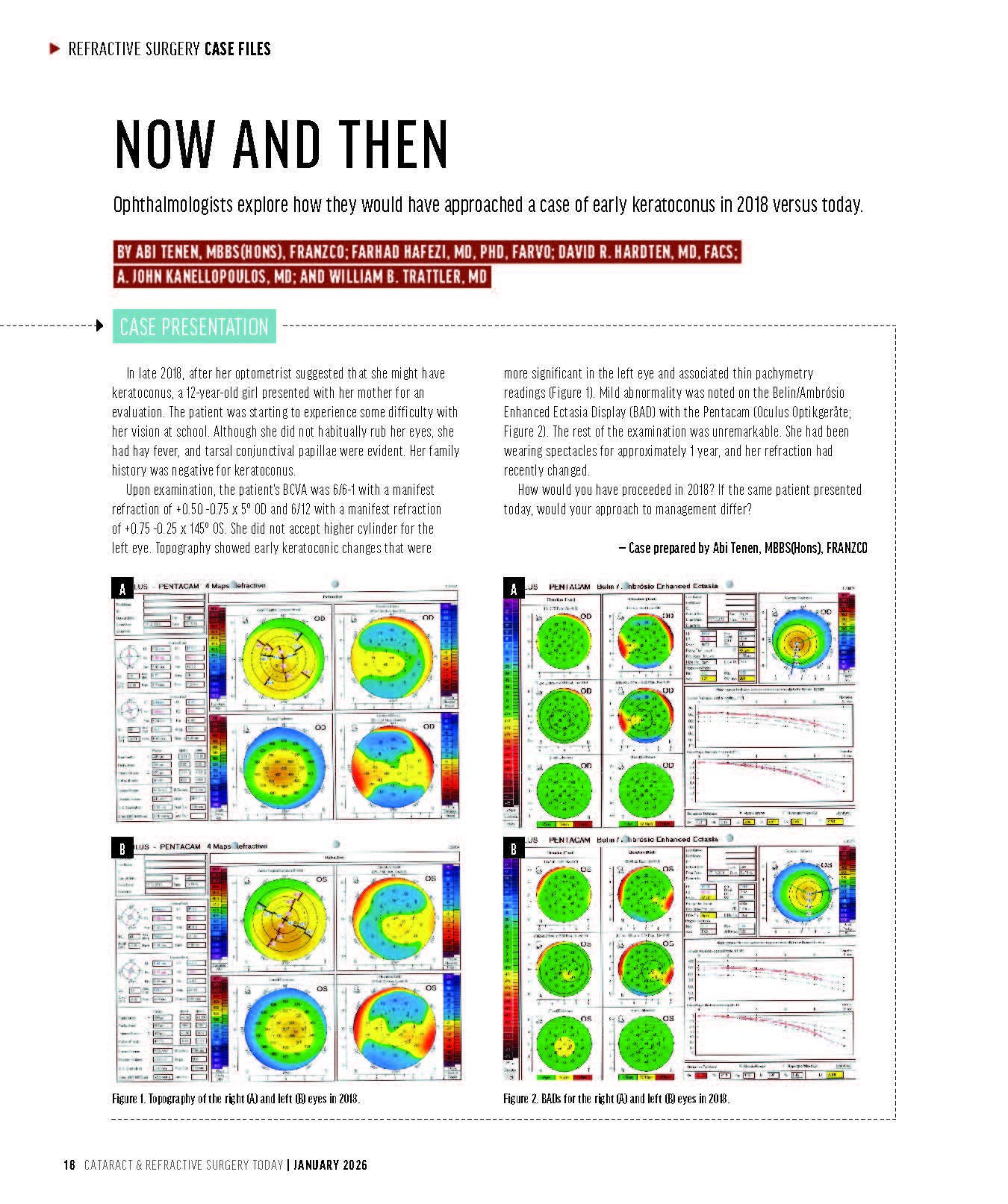
Among the contributors is Prof. Farhad Hafezi, MD, PhD, FARVO, Medical Director of the ELZA Institute, whose section focuses on the early identification and timely treatment of keratoconus in children. Drawing on long-term clinical experience and published pediatric data, Prof. Hafezi emphasizes that young patients exhibit a high risk of rapid disease progression, often before conventional criteria for documented progression are met.
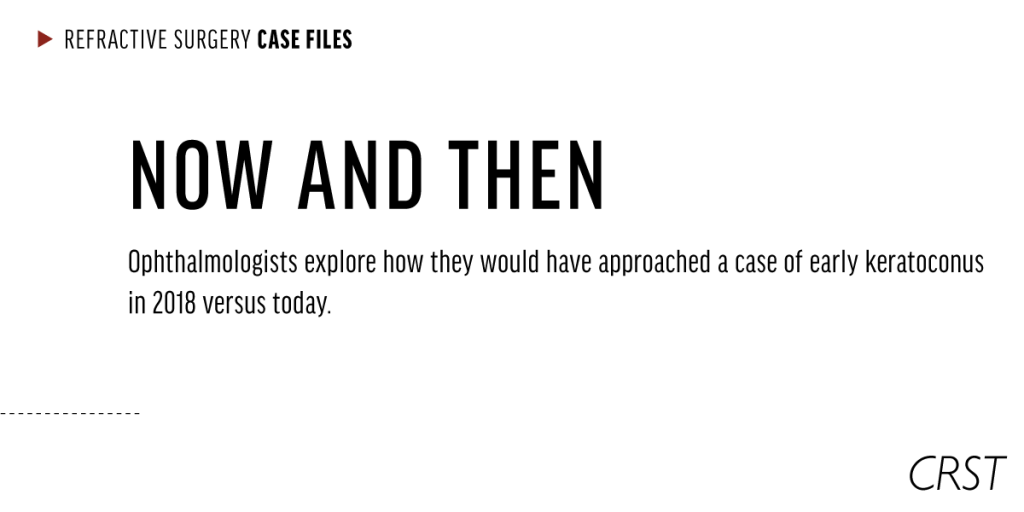
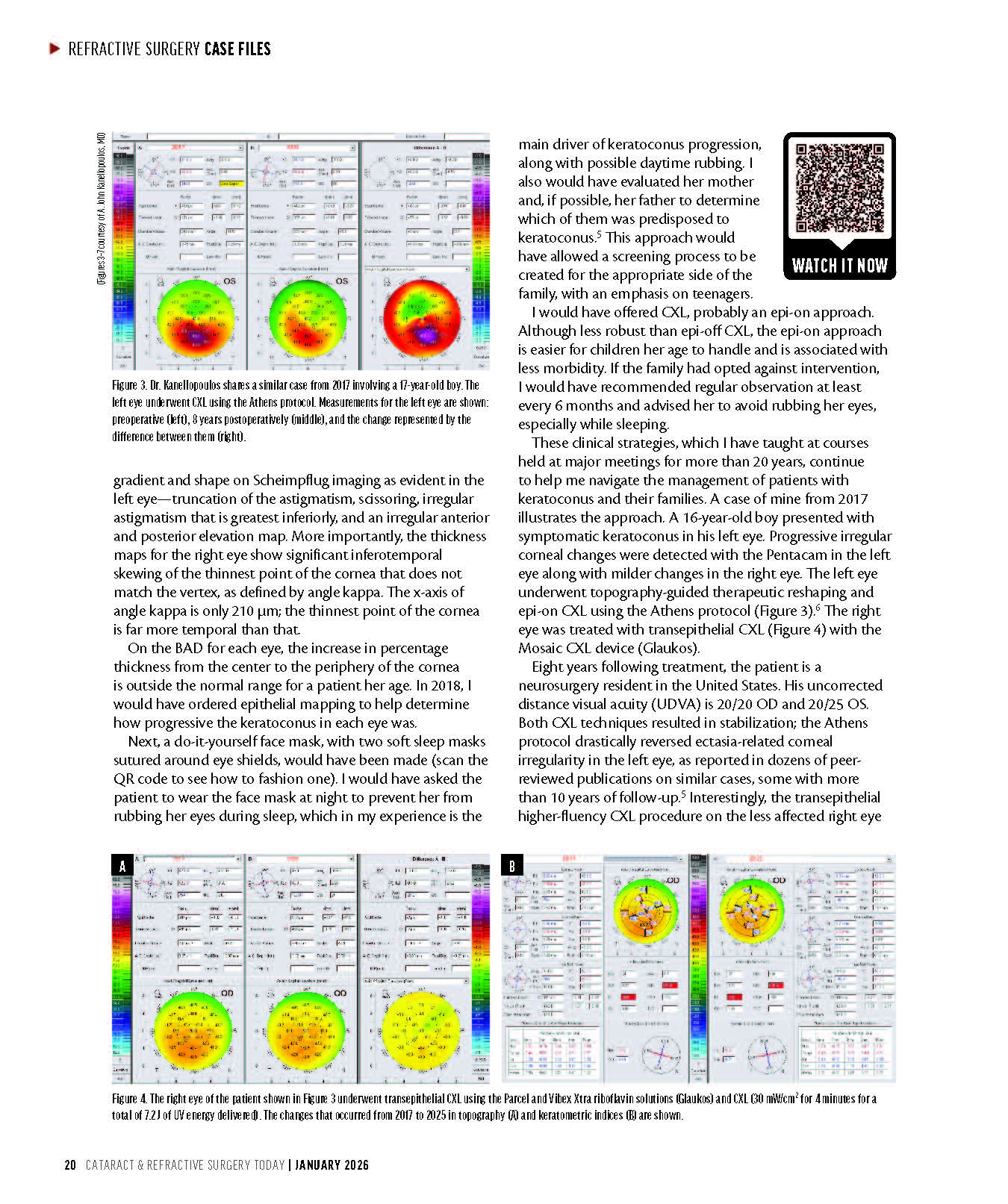
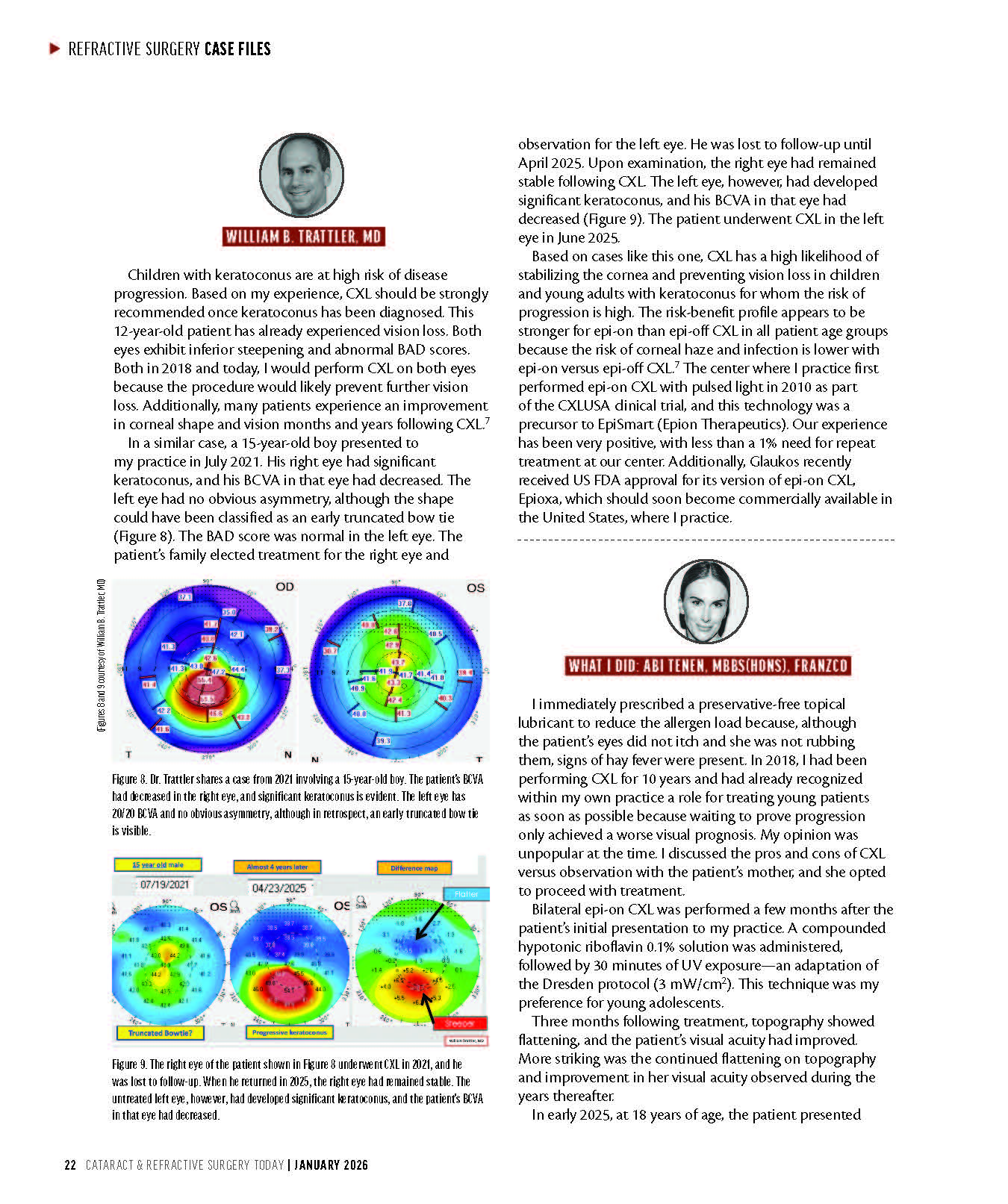
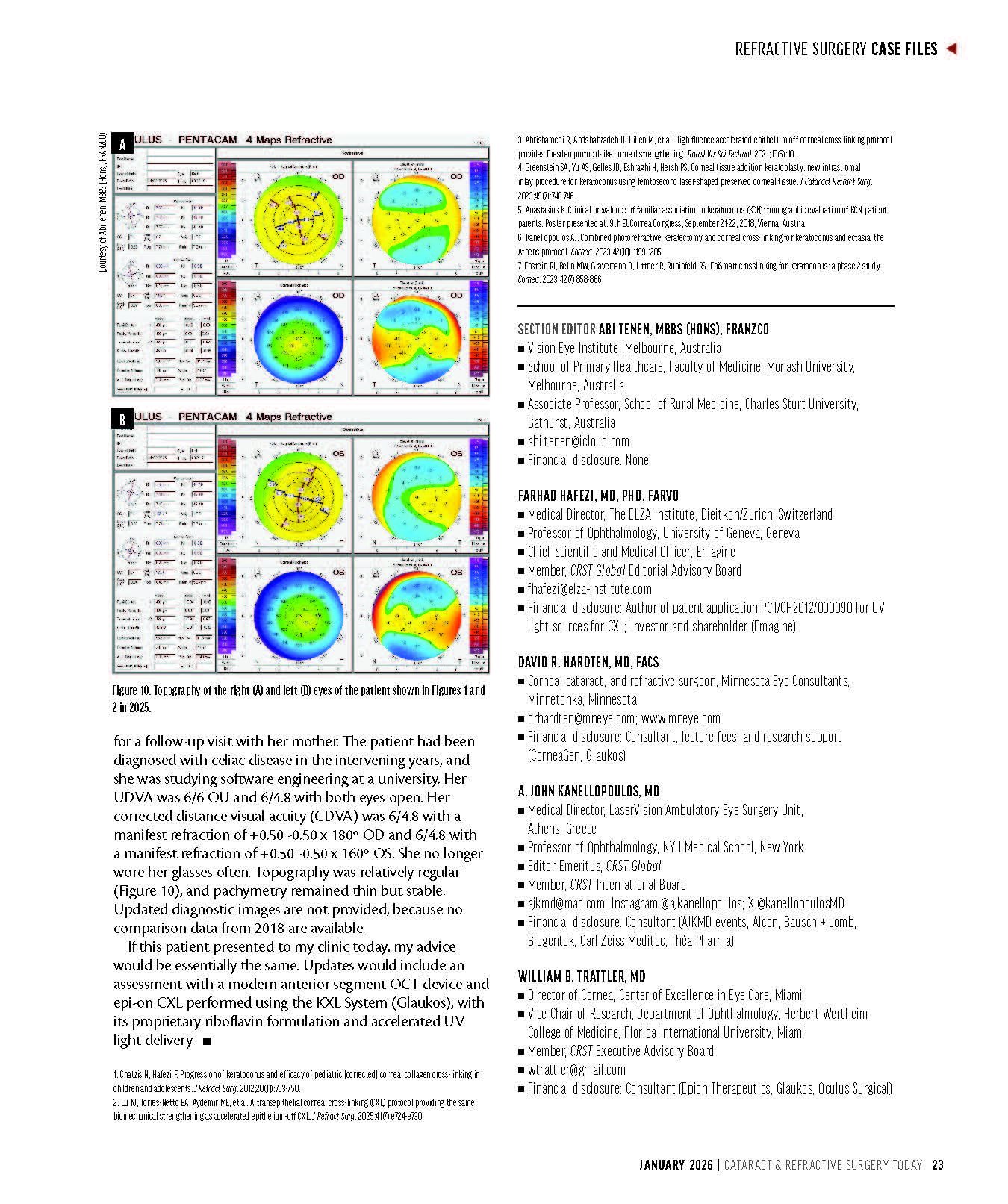
The case discussed involves a 12-year-old patient with early tomographic signs of keratoconus and thin corneal pachymetry. In 2018, management relied on Scheimpflug tomography and biomechanical assessment, with a preference for standard epithelium-off CXL to achieve maximal corneal strengthening. Since then, improvements in diagnostic resolution—particularly epithelial thickness mapping using anterior segment OCT—have enabled earlier and more confident detection of disease activity.
In the CRST article, Prof. Hafezi describes how current management would differ. For early or subclinical disease, less invasive epithelium-on accelerated CXL protocols may be selected, offering biomechanical efficacy comparable to conventional approaches while reducing patient burden. For more advanced disease, high-fluence accelerated CXL protocols delivering increased total energy over shorter treatment times are discussed as a means of achieving Dresden-equivalent corneal stiffening.
A central message of the article is the shift from delayed intervention toward immediate treatment upon diagnosis in pediatric keratoconus. This change reflects accumulated evidence that waiting for documented progression in young patients often results in avoidable visual loss. The forthcoming second global keratoconus consensus, referenced in the discussion, supports this proactive strategy, with the majority of corneal specialists now recommending early CXL in children.
The contribution in Cataract & Refractive Surgery Today illustrates how keratoconus management has moved from uniform protocols toward optimized, individualized treatment selection based on age, disease stage, and corneal characteristics.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}