Dr. Emilio de Almeida Torres-Netto, MD, PhD, FEBO, FWCRS, corneal and cataract-refractive surgeon at the ELZA Institute, has recently published an invited article in The Ophthalmologist exploring how corneal cross-linking (CXL) has evolved from a single standardized protocol into a personalized therapeutic platform. In Personalizing Corneal Cross-Linking (January 2026), Dr. Torres-Netto examines how tailored CXL strategies can be applied across real-world clinical scenarios, from patients with good vision to cataract surgery planning and advanced corneal irregularity.
Personalizing Corneal Cross-Linking: From “Dresden” to Patient-Specific Strategy
Corneal cross-linking (CXL) started as a single, standardized intervention: the “Dresden protocol.” Today, it is better understood as a treatment platform that can be adapted to disease stage, corneal phenotype, epithelial behavior, and refractive context. The January 2026 article by Torres-Netto frames this shift through three practical clinical scenarios: (1) patients with good vision, (2) keratoconus with cataract, and (3) markedly irregular corneas where both corneal stability and optical quality are relevant in planning.
Scenario 1: Good vision—prioritizing epithelial integrity and risk reduction
Historically, epithelium-on (epi-on) CXL has underperformed compared to epithelium-off (epi-off) CXL because the epithelium limits stromal riboflavin availability and restricts oxygen diffusion—both central to the photochemical cross-linking reaction. Earlier transepithelial approaches were also frequently constrained by fixed fluence strategies that did not consistently compensate for reduced stromal oxygen and riboflavin availability.
The article outlines how modern epi-on concepts attempt to address these limitations through protocol design (including optimized riboflavin formulations, oxygen dynamics, and fluence-adjusted UV delivery), aiming to narrow the efficacy gap while retaining the clinical advantages of epithelial preservation. In appropriately selected patients, maintaining the epithelium can reduce postoperative pain and minimize epithelial-defect–related risks, supporting a lower-disruption approach for those with good baseline vision or slower progression.
Where epi-on strategies may be particularly relevant (as summarized in the article):
- Patients with fragile or slow-healing epithelium
- Individuals at increased infection risk
- Those with ocular surface disease or limited postoperative compliance
- Patients with good vision and a low rate of progression
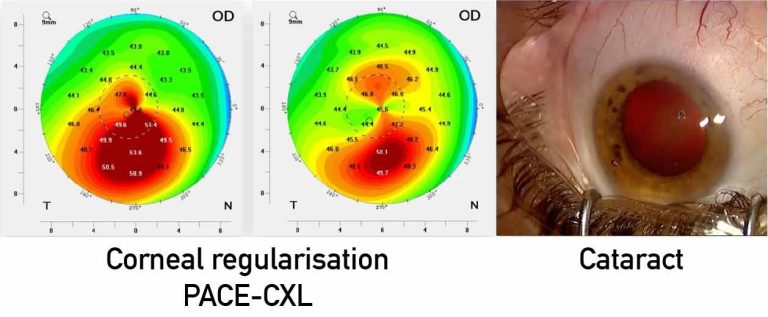
Scenario 2: Keratoconus with cataract—optimizing the cornea to improve biometry
Patients with cataract and corneal ectasia pose refractive planning challenges because irregular astigmatism can degrade keratometric reliability and reduce the predictive accuracy of IOL calculations. The practical point emphasized is that when corneal irregularity—particularly within the central cornea and visual axis—meaningfully affects measurements, corneal optimization before cataract surgery can improve biometric quality and refractive predictability.
The article discusses a range of possible corneal optimization strategies used in ectatic eyes, including reshaping approaches (such as intracorneal ring strategies, including tissue-based options) and customized CXL concepts intended to target focal biomechanical weakness and encourage corneal regularization. This staged logic is presented as a way to reduce postoperative refractive “surprises” by improving the inputs used for IOL power calculations.
When corneal irregularity has minimal impact on IOL calculations—or when staged procedures are impractical—the article notes that cataract surgery can reasonably take precedence, with corneal optimization considered later if required. In such cases, careful assessment of contact lens history remains important to avoid distorted preoperative measurements.
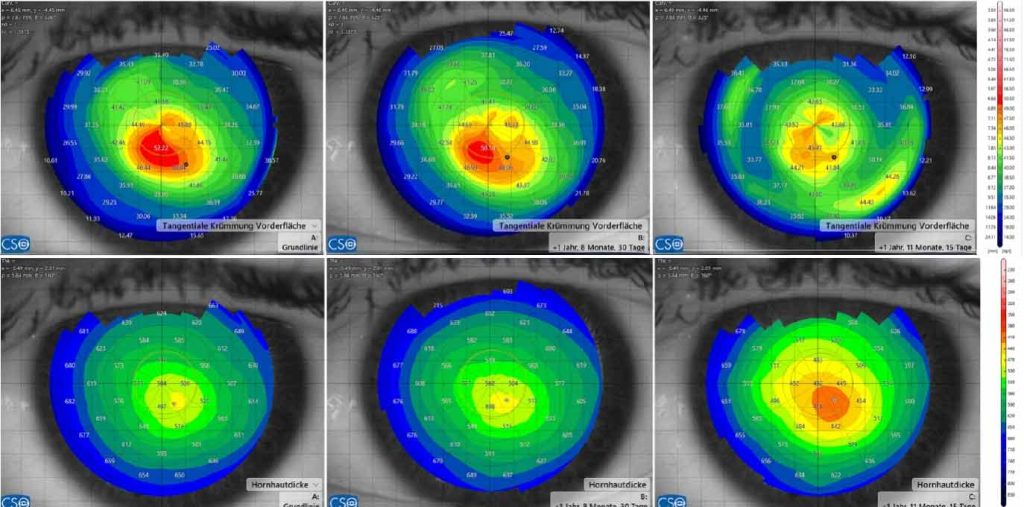
Scenario 3: Markedly irregular corneas—combining customized CXL and excimer enhancement
For eyes with marked asymmetry or irregularity, the article describes a staged or combined approach intended to address both stability and optical quality. Customized CXL concepts (including PTK-assisted customized epi-on strategies) are presented as methods to selectively reinforce biomechanical weakness to encourage a more regular corneal profile without removing stromal tissue.
Once corneal stability is established, a topography-guided or wavefront-guided excimer laser enhancement may be considered in carefully selected cases with adequate thickness and biomechanical reserve. The article highlights an additional planning concept: treatment strategies that incorporate both anterior and posterior corneal optics may reduce the amount of tissue ablation required to achieve meaningful optical improvement—an especially relevant consideration in ectatic corneas where tissue preservation is paramount.
From standardization to personalization: rethinking CXL
CXL should no longer be viewed as a one-size-fits-all procedure. The personalization paradigm described in the article centers on selecting the appropriate CXL approach, timing, and adjuncts according to the individual clinical context, including:
- Progression rate and disease severity
- Epithelial behavior
- Patient age and visual expectations
- Refractive planning needs (including cataract surgery)
- Corneal regularity and optical requirements
Beyond stabilization
In selected cases, CXL can contribute to optical rehabilitation—particularly when used as part of a staged strategy that may include customized cross-linking, tissue-based ring approaches, or excimer laser refinement. A key advantage emphasized is CXL’s tissue-sparing profile: because CXL removes no tissue and adds no permanent implant, it can be integrated into sequential strategies designed to refine both biomechanics and visual quality.
From ultra-thin corneas (where individualized approaches such as sub400 are referenced in the source article) to advanced irregularity where visual rehabilitation is pursued with combined strategies, the broader message is consistent: contemporary CXL is increasingly a personalized therapeutic platform, not a single protocol.
Read the full article: Personalizing Corneal Cross-Linking (The Ophthalmologist, January 2026)