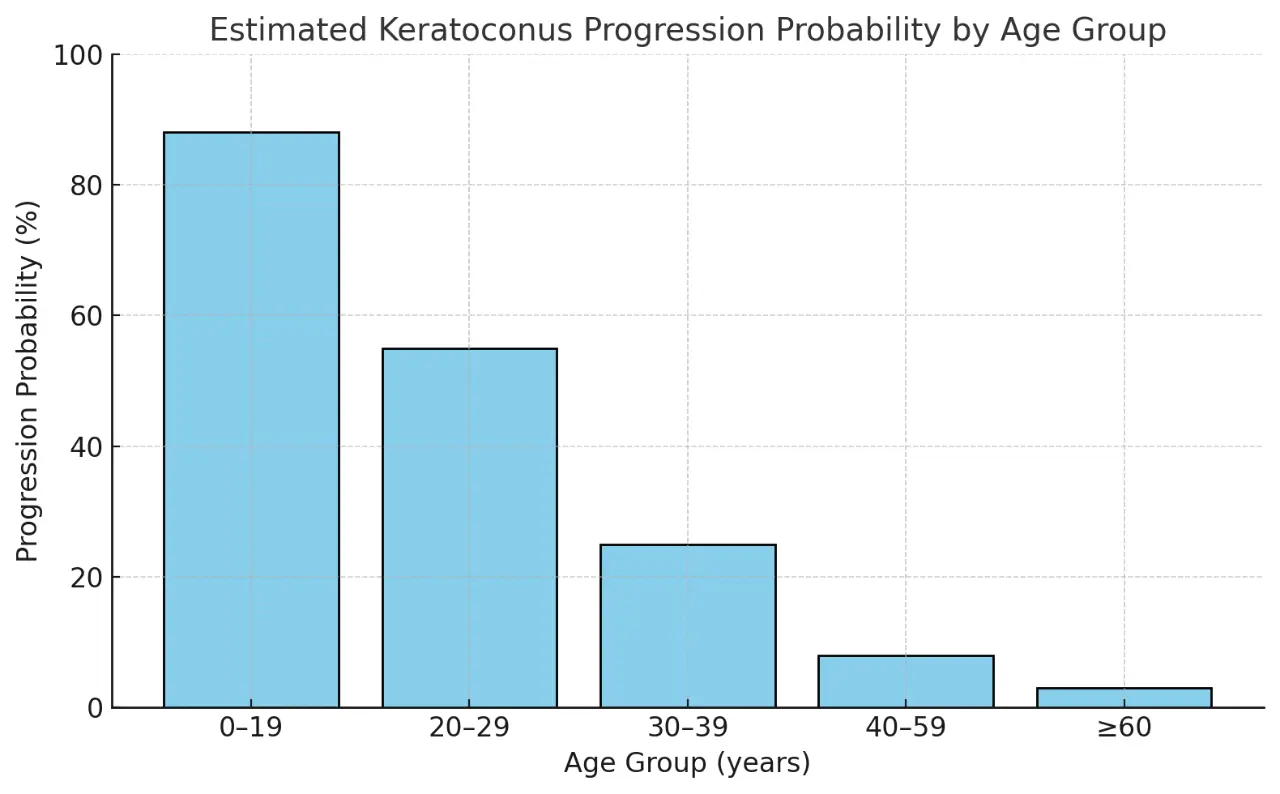
Keratoconus in children and adolescents progresses rapidly, with studies showing that approximately 9 out of 10 children diagnosed with keratoconus will experience disease progression. Immediate treatment with corneal cross-linking (CXL) upon diagnosis is recommended to halt disease progression and preserve vision.
For detailed information, please visit our dedicated Pediatric Keratoconus page.
Chatzis, N., & Hafezi, F. (2012). J Refract Surg, 28(11), 753–758.
Mazzotta, C., et al. (2018). Ophthalmology, 125(9), 1230-1236.
Kollros, L., et al. (2023). Cornea, 42(4), 450-457.
Wollensak, G., Spoerl, E., & Seiler, T. (2003). Am J Ophthalmol, 135(5), 620–627.
In adults, keratoconus progression often slows or stabilizes with age due to natural collagen stiffening, usually around 35–40 years of age. By contrast with children, in adults, CXL is generally advised only after documented progression is confirmed through corneal topography/tomography imaging or vision changes. Historical data, such as changes in prior spectacle prescriptions, can aid in assessing progression. However, the nature of keratoconus is different for each individual, so regular monitoring remains essential.
Mechanical trauma from habitual eye rubbing significantly accelerates keratoconus progression by weakening corneal collagen. The ELZA Institute is among the world leaders in researching this association, publishing multiple key studies demonstrating the biomechanical effects of eye rubbing on corneal stiffness and ectasia development.
Eye rubbing with finger
Eye rubbing with knuckles
Hormones such as oestrogen and thyroid hormone affect corneal biomechanics. Elevated oestrogen during pregnancy softens corneal tissue, increasing progression risk, while hypothyroidism has been linked to accelerated keratoconus through effects on collagen cross-linking enzymes. ELZA’s research has been foundational in establishing these links.
Cross-linking decisions depend on multiple factors, including age, disease progression, and modifiable risks such as eye rubbing and hormonal status. At ELZA, we continuously lead research efforts to improve understanding and outcomes in keratoconus management.
Get in touch
During office hours.
Email us.
Make an appointment, and come to see us.
Thank you for writing a review on google.
Contact us here, we will get in touch with you.
Zoom online consultation for our international patients.
Contact us here, we will get in touch with you.
Contact us here, we will get in touch with you.
Stay informed & get the newsletter
You have successfully joined our subscriber list.
Newsletter abonnieren & informiert bleiben
Sie haben sich erfolgreich in unsere Abonnentenliste eingetragen.
Bitte bestätigen Sie Ihr Abonnement, indem Sie auf den Link in der E-Mail klicken, die wir Ihnen gerade geschickt haben.
{kind=link}
{kind=link}
{kind=link}