Treating infectious keratitis with CXL is not like treating keratoconus with CXL. We recently had to write a letter to the journal, Ophthalmology, to point out the flaws in a recent publication in the journal.
The paper in question used one of the most exciting aspects of corneal cross-linking (CXL), a procedure called photoactivated chromophore for keratitis-CXL, or PACK-CXL, as a method of treating fungal keratitis. In their study, 111 patients received either topical antifungal agents (either natamycin 5% or amphotericin 0.15%) with or without PACK-CXL. However, in the end, they concluded, “there appears to be no benefit of adjuvant CXL in the primary treatment of moderate filamentous fungal ulcers, and it may result in decreased visual acuity.”
We believe they made a basic error which meant that an inadequate amount of UV irradiation (fluence) was applied during PACK-CXL to treat fungal infections.
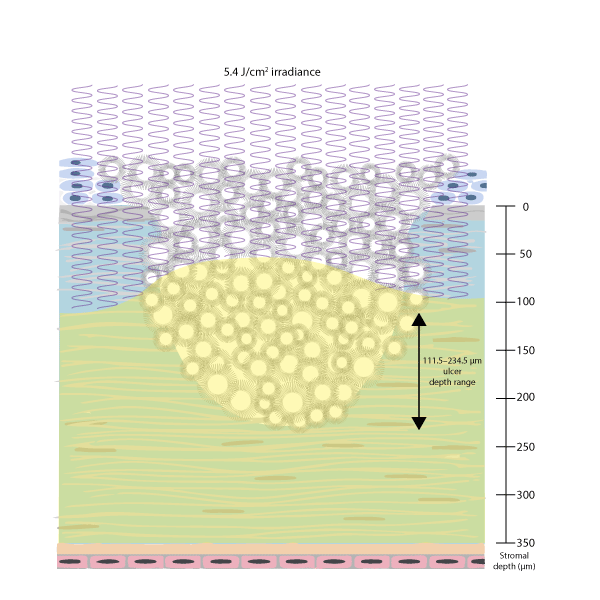
This paper was flawed. It lacked basic details like baseline ulcer size and UV fluence applied. However, looking at the methods section, they cited the classic keratoconus cross-linking “Dresden protocol” (30 minutes of 0.1% riboflavin instillation, followed by 30 minutes of 3 mW UV illumination for a total fluence of 5.4 J/cm2), so we figured it was safe to assume that was used here.
But the Dresden protocol is totally inadequate for treating infectious keratitis, whether it is bacterial or fungal. To explain why, we need to explore what happens when a cornea is cross-linked.
When stroma that is saturated with riboflavin is hit by a UV photon, the riboflavin gets activated, reacts, generates a reactive oxygen species “ROS” which can cross-link the molecules of the stroma together, or attach the cell membranes and nucleic acids of any pathogens present. But it gets consumed. It’s challenging for UV light to penetrate much deeper, as the riboflavin acts as a shield (that gets consumed) against it penetrating further. This is good in many respects, as it protects the corneal endothelial cells at the base of the cornea from being damaged by UV irradiation. But it also means that UV energy absorption decays in a logarithmic manner. The amount of UV energy delivered by the Dresden protocol therefore only cross-links the first 100 µm.
So how deep were these patients’ ulcers? The Methods section says that eyes with “involvement of the posterior one-third of the stroma,” and “central pachymetry less than 350 mm” were excluded, and that 46% and 68% of CXL treated patients (with natamycin and amphotericin, respectively) had ulcer depths of 33–67% of the depth of the stroma.
Let’s do some arithmetic to find what would be the shallowest-possible ulcer depth (and therefore had the greatest chance of successful treatment with a PACK-CXL protocol that treats just the top 100 µm of the cornea).
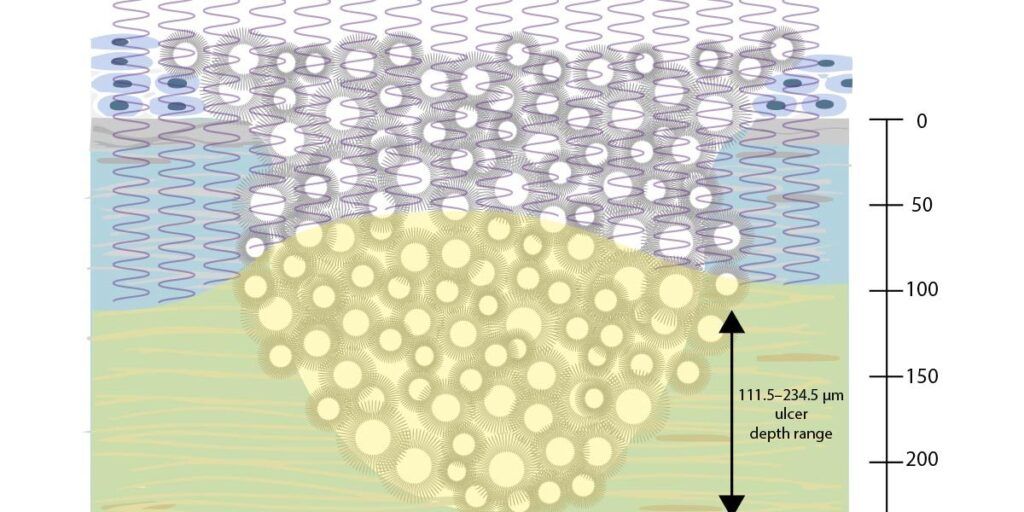
If the thinnest cornea was 350 µm in the study, and the shallowest ulcer depth range was 33–67%, this means that the ulcer depths range from 111.5–234.5 µm – and therefore thicker corneas would have even deeper ulcers.
Finally, this all assumes that the cornea is a keratoconic one, not one with an ulcer – which is opaque, meaning that it is even harder for UV light to penetrate into the cornea. All in all, this means that even in the best-case scenario, not enough UV energy was delivered into the cornea to treat all of the infection.
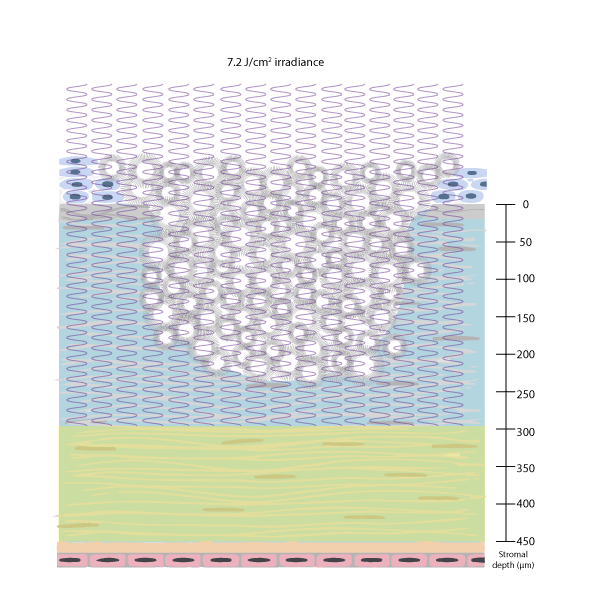
We have already shown that PACK-CXL is more effective at killing bacteria when higher UV fluences are used, and we are seeing in our ongoing clinical trial that the effectiveness of PACK-CXL with a total fluence of 7.2 J/cm² is similar to that of antimicrobial therapy. For these reasons, we believe the authors of this paper used an inadequate fluence to treat these patients’ fungal ulcers.
References
- Hafezi F, Torres-Netto EA, Hillen MJP. Re: Prajna et al.: Cross-Linking–Assisted Infection Reduction: a randomized clinical trial evaluating the effect of adjuvant cross-linking on outcomes in fungal keratitis. Ophthalmology. 2020. Aug 13. Online ahead of print.
- Prajna NV, Radhakrishnan N, Lalitha P, et al. A randomized clinical trial evaluating the effect of adjuvant cross-linking on outcomes in fungal keratitis. Ophthalmology. 2020;127: 159e166.
- Kling S, Hufschmid FS, Torres-Netto EA, et al. High fluence increases the antibacterial efficacy of PACK cross-linking. Cornea. 2020;39:1020e1026.