In laser refractive surgery, corneal tissue is removed with a laser to correct the refractive error or astigmatism. A normal cornea tolerates this easily. However, if too much tissue is removed, or if the cornea is endangered by other causes (hormones, pre-existing or undetected disease), then ectasia following LASIK, PRK and SMILE can still occur years after surgery. This ectasia is very similar to keratoconus and even has the same symptoms.
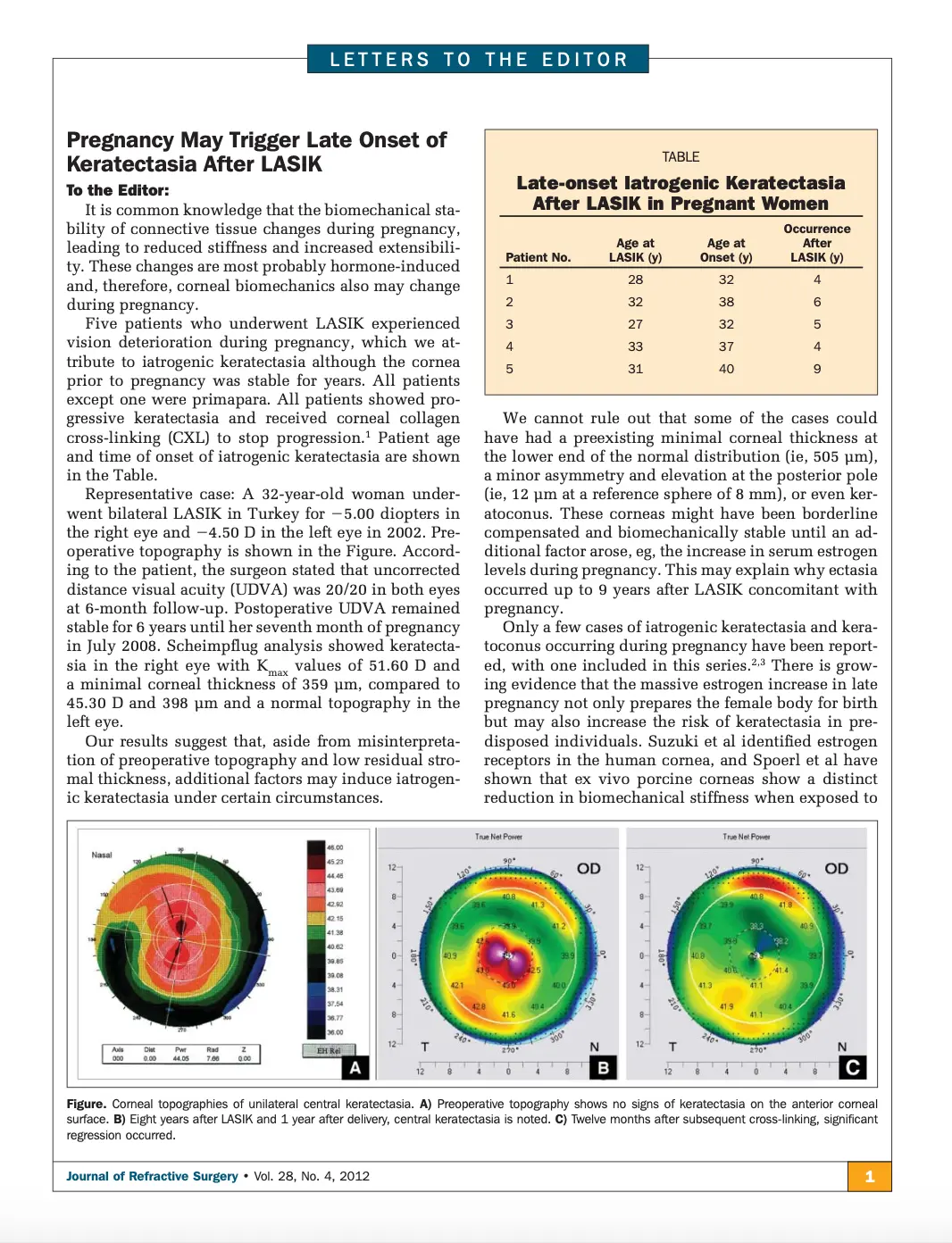
We were the first to show in 2012 that this ectasia can even occur 9 years after LASIK. It is all the more important that the surgeon has a great deal of experience in detecting such risk factors before surgery.
Ectasia developing after LASIK, PRK, or SMILE – often described as “man-made” keratoconus – belongs to the family of corneal ectasias alongside keratoconus and pellucid marginal degeneration (PMD). Before 2007, this complication was one of the most devastating outcomes of refractive surgery, with corneal transplantation as the only available treatment. This invasive procedure required general anesthesia and carried significant risks, including graft rejection and prolonged recovery times.
In 2007, Prof. Farhad Hafezi and colleagues published the world’s first successful clinical study demonstrating the efficacy of corneal collagen cross-linking (CXL) to halt the progression of post-LASIK ectasia. This seminal paper, cited over 600 times, laid the foundation for CXL to become the global gold standard treatment for this previously untreatable condition.
Thanks to ELZA’s pioneering work, patients worldwide now benefit from a less invasive, safer option that stabilizes corneal structure, dramatically reducing the need for transplantation and improving quality of life. Moreover, this initial breakthrough sparked a wave of research globally, inspiring numerous groups, including ours, to refine and expand CXL protocols for post-refractive ectasia, cementing its central role in contemporary corneal therapy.
Until 2007, the only option for treating ectasia after LASIK and PRK was corneal transplantation (keratoplasty). This operation is serious (it requires general anaesthesia) and carries the risk of rejection.
However, in 2007, the world saw the very first patients with post-LASIK ectasia successfully treated with CXL. Since then, CXL has become the global gold standard for the treatment of this disorder.
2007: World's first successful treatment
of ectasia after LASIK
2012: Our successful long-term results
Get in touch
During office hours.
Email us.
Make an appointment, and come to see us.
Thank you for writing a review on google.
Contact us here, we will get in touch with you.
Zoom online consultation for our international patients.
Contact us here, we will get in touch with you.
Contact us here, we will get in touch with you.
Stay informed & get the newsletter
You have successfully joined our subscriber list.
Newsletter abonnieren & informiert bleiben
Sie haben sich erfolgreich in unsere Abonnentenliste eingetragen.
Bitte bestätigen Sie Ihr Abonnement, indem Sie auf den Link in der E-Mail klicken, die wir Ihnen gerade geschickt haben.